

By Ruth Waitzberg and Bruce Rosen, Myers-JDC-Brookdale Institute
Israel provides universal coverage to citizens and permanent residents as part of its national health insurance law. Residents choose from four competing nonprofit health plans that provide a mandated benefit package, including hospital, primary, specialty, mental health, and maternity care, as well as prescription drugs and other services. There are no deductibles, but some cost-sharing is required for specialist visits and prescription drugs. The compulsory insurance system is funded primarily through a national income tax and an income-related health tax. Most citizens also purchase voluntary health insurance for medications not covered by the benefit package and for faster access and greater provider choice. Almost all governmental health functions are organized by the Ministry of Health, which has regional and district health offices.1
Sections
How does universal health coverage work?
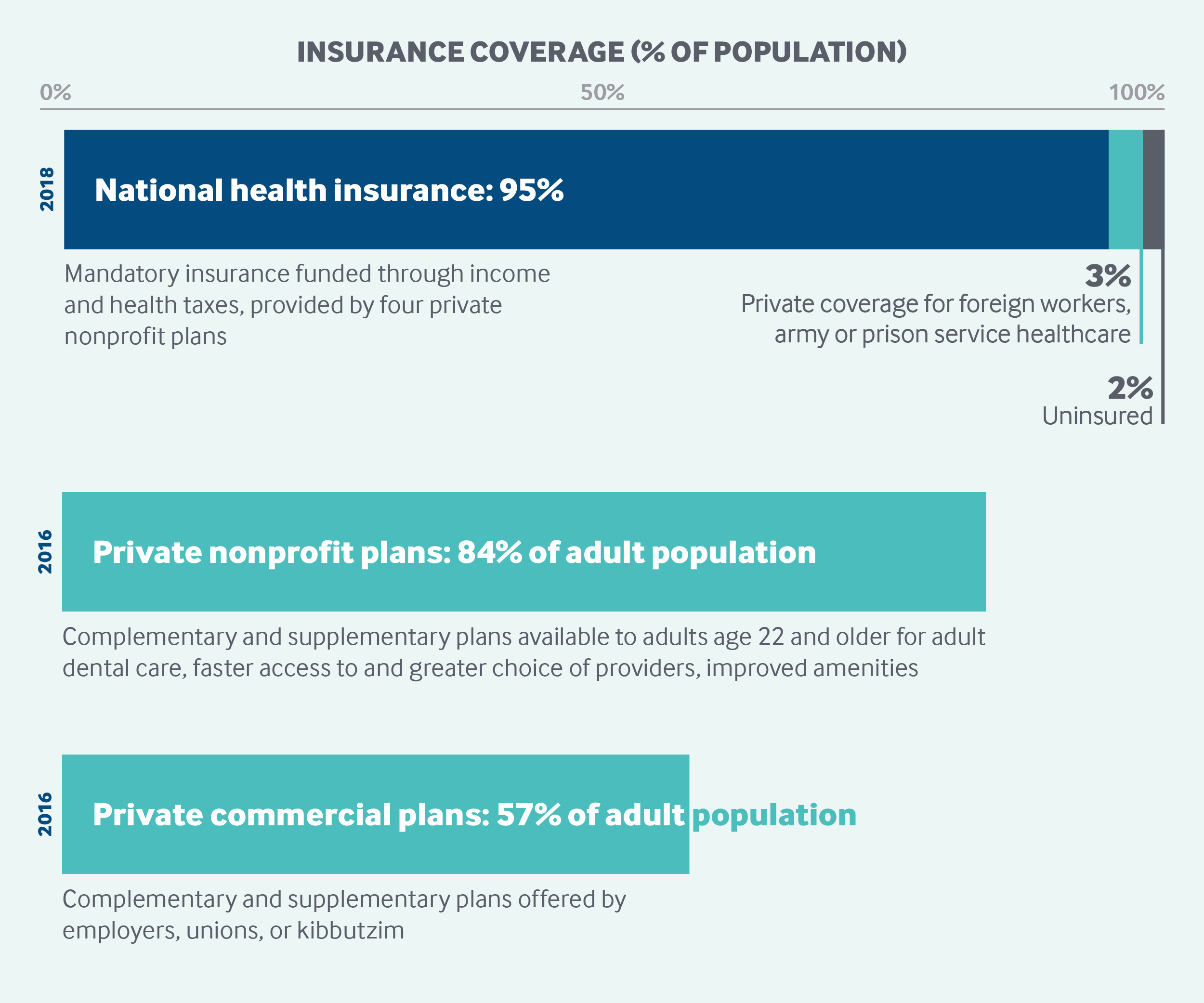
Since 1995, Israel’s National Health Insurance (NHI) law has ensured universal coverage for citizens and permanent residents. As the law states, "Health insurance…shall be based on principles of justice, equality and mutual assistance." Under this commitment, every resident is entitled to health care services.
Residents are free to choose one of four competing nonprofit health plans that must cover anyone who applies. Every resident has a right to receive all services included in the benefit basket that is mandated by the government, subject to medical discretion. While residents also have the right to receive services at a reasonable quality level, within a reasonable period of time, and at a reasonable distance from their home, no formal definition of “reasonable” exists, and there is no penalty for health plans that fail to comply.
Some populations are excluded: soldiers, who receive health care directly from the army; inmates, who receive care from the Israel Prison Service; documented and undocumented foreign workers, whom employers are required to enroll in private insurance programs; and undocumented migrants, temporary residents, and tourists.2
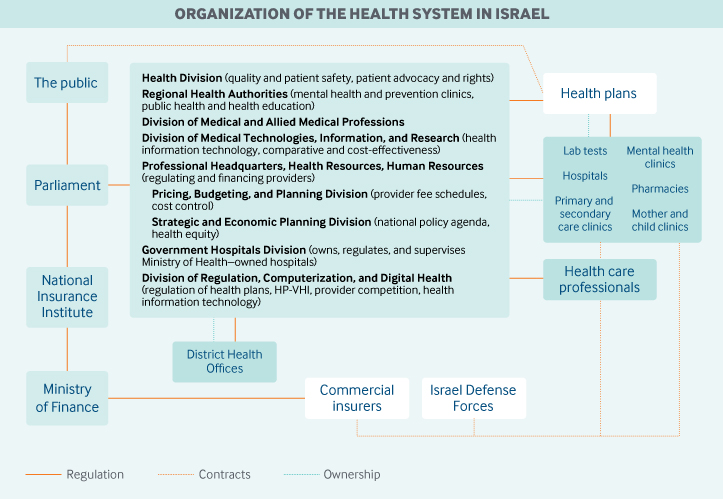
Role of government: The national government, through the Ministry of Health, is responsible for population health and the overall functioning of the health care system. It supervises and works with the NHI health plans and owns and operates a large network of maternal and child health centers, about half of the nation’s acute care bed capacity, and about 80 percent of its psychiatric bed capacity.3 In addition to financing insurance, the national government funds public-health services and is directly responsible for the provision and funding of certain other health services, including prenatal and preventive care, infant developmental tests, communicable disease surveillance, screenings, and institutional long-term care.
Local governments have limited involvement in health care provision. Accordingly, nearly all governmental health functions are organized by the national Ministry of Health, which comprises a network of regional and district health offices.
Various advisory bodies, including the following, counsel the Ministry of Health and handle specific responsibilities:
- The National Health Council, a public advisory council, advises on prominent health policy issues.
- The Benefits Package Committee provides guidance on the prioritization of new technologies for inclusion in the NHI benefit package and carries out health technology assessments for new medications.
- Various national councils provide external professional input in specific areas, such as trauma care, mental health, and women’s health.
- The Ministry of Finance’s Insurance and Capital Markets Division regulates commercial voluntary health insurance.
- An ombudsman’s office helps citizens realize their rights under the NHI law. In addition, there are various nongovernmental patient advocacy organizations, many of which focus on particular diseases.
- The Scientific Council of the Israel Medical Association is responsible for specialty provider certification programs and examinations, in coordination with the Ministry of Health.
- The Council for Higher Education is responsible for the authorization, certification, and funding of all university degree programs, including the training of health care professionals.
- A joint Ministry of Health – Ministry of Finance committee sets the fees for hospitals, other providers, and services. These ministries are also engaged in cost-control efforts, but responsibility for cost containment is distributed over a number of different departments.
The Ministry of Health also has units that monitor quality and patient safety in hospitals and additional settings, provide national leadership in health information technology, promote health equity, and address issues of competition within health care.
Role of public health insurance: In 2017, national health expenditures accounted for 7.4 percent of GDP, a figure that has remained stable during the last two decades. In 2017, 63 percent of health expenditures were publicly financed, a share that is one of the lowest among Organisation for Economic Co-operation and Development (OECD) countries.
Israel’s NHI system is funded primarily through an earmarked, income-related health tax (5% of income for individuals age 22 and older) in combination with general government revenues, which are funded primarily through progressive income taxation paid by individuals. Married women, children, and all those who are excluded from the NHI (such as soldiers) are exempt from the health tax.
The government distributes the NHI budget among the four health plans primarily through a capitation that accounts for sex, age, geographic distribution of their members and five chronic, expensive-to-treat diseases.
Role of private health insurance: Private, voluntary health insurance financed 14 percent of national health expenditures in 2016.4 Residents can obtain voluntary health insurance from the four NHI nonprofit plans as well as from for-profit commercial plans. The NHI plans cannot reject applicants, and premiums are based on age only. Commercial private plans tend to be more comprehensive, more individually tailored, and more expensive, and can be purchased by individuals or groups, such as employers, unions, or kibbutzim.
Nearly all individuals purchase private insurance from either the NHI plans or commercial insurers, or both. In 2016, 84 percent of Israel’s adult population was enrolled in an NIH private insurance plan, and 57 percent were enrolled in a commercial private insurance plan.5
Voluntary health insurance plays a complementary role, covering benefits excluded from the NHI scheme (dental care for adults, certain medications, alternative medicines), as well as a supplementary role, expanding access to NHI-covered benefits, offering access to private providers, and providing improved amenities and faster access to care. The high number of those with voluntary health insurance coverage reflects a general lack of confidence in the NHI system’s capacity to fully fund and deliver all services needed in cases of severe illness.
Services covered: The mandated NHI benefit package includes the following:
- hospital care
- primary and specialty care
- prescription drugs
- certain preventive services
- mental health care
- dental care for children and the elderly aged 75+
- diagnostic exams
- maternity care
- allied medical care (physiotherapy, occupational therapy, nutrition, speech therapy)
- some durable medical equipment (wheelchairs, orthopedic aids)
- limited coverage of palliative and hospice services.6
Dental care for adults, optometry, and hearing aids are excluded.
Means-tested institutional long-term care, infant developmental screenings and vaccinations, and postpartum care like breastfeeding guidance are covered by the Ministry of Health, but separately from NHI.
Cost-sharing and out-of-pocket spending: In 2016, out-of-pocket spending accounted for 22 percent of national health expenditures.7 Most of this was for voluntary health insurance (38%), adult dental care (22.5%), and pharmaceuticals (15%). The remainder was for other services not included in the NHI benefit package, including vision care and medical equipment, as well as cost-sharing for NHI-covered services.
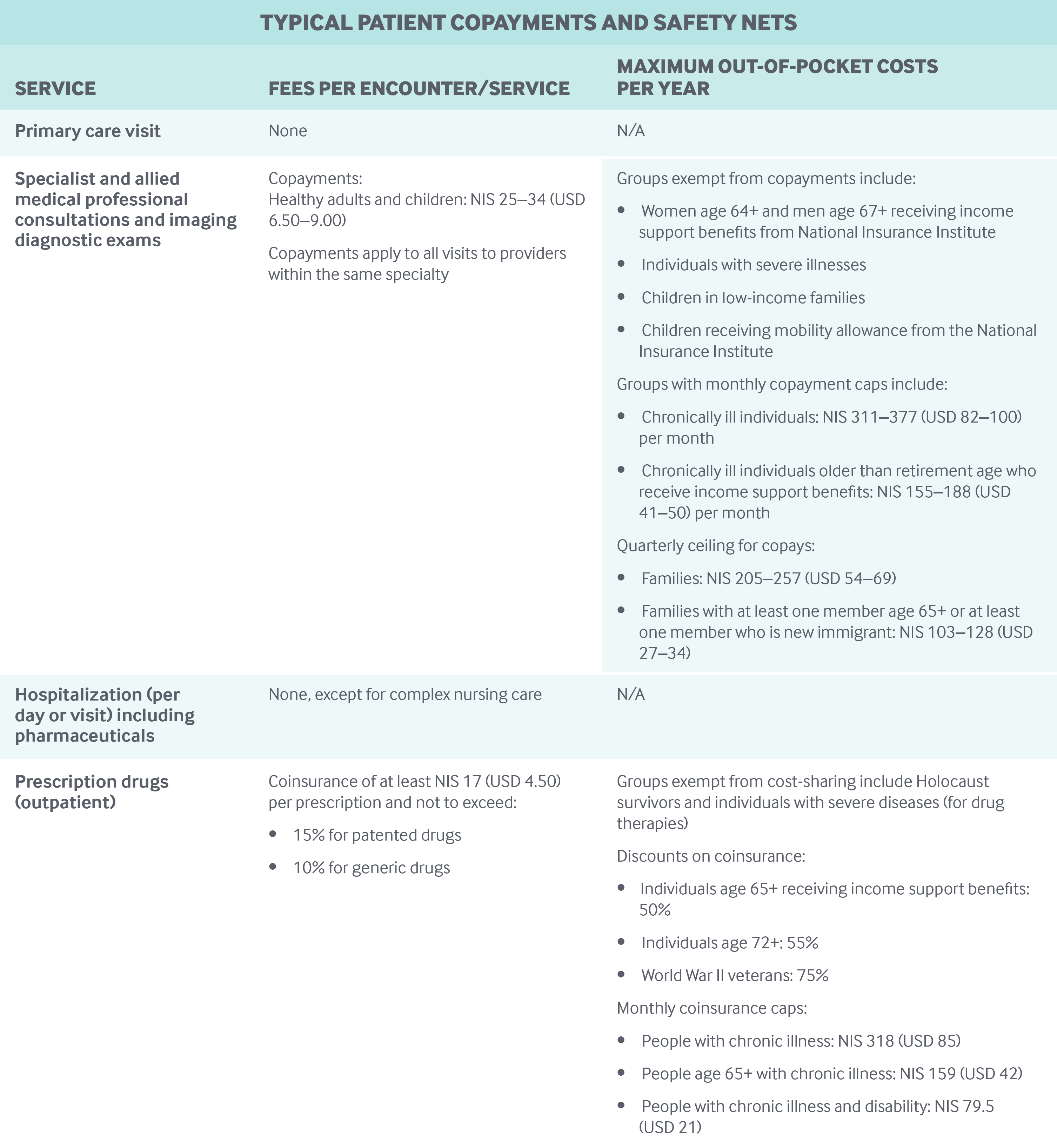
NHI health plans are allowed to impose user charges for certain services. These include a flat quarterly copayment rate for visits to specialists and allied medical professionals and for imaging diagnostic exams; a user charge for after-hours emergency care in the community; and coinsurance for pharmaceuticals (see table below). User charges, which are regulated by the Ministry of Health, constituted about 6.5 percent of health plan income in 2016. There are no copayments for primary care visits, preventive care, cancer screenings, or hospital admissions. There are also no quarterly or annual deductibles with NHI coverage.
Safety nets: Safety nets include an annual cap on the health tax at NIS 43,370 (USD 11,565). In addition, individuals with low incomes (60% of average income or less) pay a reduced health tax rate of 3 percent, compared to 5 percent paid by individuals with higher incomes. The unemployed and others without income pay a minimum flat health tax of approximately NIS 100 (USD 27) per month.8
Israel also has caps on user charges and discounts for older adults, the chronically ill, and other vulnerable populations, as shown in the table below.
How is the delivery system organized and how are providers paid?
Physician education and workforce: Israel has six medical schools, which are all part of public, nonprofit universities. The number of medical schools and students is regulated by the higher education council. As of 2015, more than half (58%) of Israeli physicians under age 65 had completed their medical studies abroad. Annual tuition, heavily subsidized by the government, is approximately NIS 11,100 (USD 3,000) for the first three years and NIS 14,800 (USD 4,000) for the next three years.
To address physician shortages in the entire country and in remote areas in particular, the government introduced two measures in 2011: it increased the number of physician positions in all hospitals throughout the country and introduced financial incentives (onetime bonuses and salary differentials) to encourage physician graduates to pursue their residencies in remote regions. The combination of these two programs has increased the number of residencies completed, especially in remote settings. Similar financial incentives encourage physicians to choose in-demand specialties, such as anesthesiology, geriatrics, and pediatric neurology.
Primary care: In 2018, 5,052 of the 38,523 licensed physicians (13%) were employed as general practitioners (GPs). The average number of GPs per capita in Israel is 0.6 GPs per 1,000 people (or 1 GP per 1,653 insured). However, this rate varies across regions and health plans (ranging from 0. 57 to 0.73).9
Most GPs contract with one of the four competing nonprofit NHI health plans. Only 5 percent have contracts with more than one health plan.10
The four NHI health plans (Clalit, Maccabi, Meuhedet, and Leumit) have different approaches to organizing care. Clalit, the largest health plan, provides most primary care in clinics that it owns and operates, and GPs are salaried employees. The typical clinic is multidisciplinary, with three-to-six GPs and several nurses, pharmacists, and other professionals. Clalit also contracts with independent physicians who tend to work in solo practices, with some access to administrative and nonphysician services at Clalit district clinics.
The other three health plans also use a mix of multidisciplinary clinics and independent primary care practices. In Maccabi (the second-largest plan) and Meuhedet, almost all of the primary care is provided by independent physicians, while in Leumit the clinic model predominates.
Members of all plans can generally choose their GP from among those on the plan’s list and can switch freely. In practice, nearly all patients remain with the same GP for extended periods.
In Clalit, each patient is registered with a GP who has responsibility for coordinating care. Clalit is also the only plan that requires gatekeeping; referrals are required for secondary care, except for five common specialties (dermatology, otorhinolaryngology, ophthalmology, orthopedics, and gynecology). In Leumit, patients are registered with a clinic rather than with a GP, and in the other two plans there is no registration.
Approximately one-third of Israel’s nurses work in community settings, primarily as salaried employees of the four NHI health plans. Their roles have been expanding beyond traditional routine nursing care (see “What innovations and reforms have recently been introduced?”). In a 2015-2016 national survey, 38 percent of frontline nurses employed by health plans identified “caring for chronically ill patients” as their main area of activity in addition to routine care, and 30 percent noted “health promotion.”11
Doctors are paid entirely by the health plans; they cannot collect additional fees from their patients.
Salaries of Clalit clinic-based physicians are set via a collective bargaining agreement with the Israel Medical Association. Capitation rates for independent physicians in all health plans are set by the plans in consultation with physicians’ associations.
Clalit and Leumit use predominantly “passive capitation,” a quarterly, per-member payment made irrespective of whether the member visited the GP in the relevant quarter. Maccabi and Meuhedet use “active capitation,” whereby payment is made only for members who visited their GP at least once during the quarter. Independent physicians also receive limited fee-for-service payments for certain procedures. Quality-related financial incentives are generally not used.
Outpatient specialty care: Outpatient specialty care is provided predominantly in community settings, either in health plan clinics or in physicians’ offices. The former tend to be integrated multispecialty clinics, while the latter tend to be single-specialty.
Patients can choose freely among community-based specialists who are contracted with their health plan. Services provided by out-of-network specialists are paid for out-of-pocket or covered by voluntary health insurance.
Most outpatient specialists are paid on an active capitation basis, plus fee-for-service for certain procedures, up to a quarterly ceiling. Rates are set by the health plans. Specialists may not “balance bill” for NHI-covered services. Nevertheless, specialists can receive patients from NHI health plans along with patients who have private voluntary health insurance, but not the same patient in both settings. For privately insured patients, specialists can set their payment rates at their discretion.
Administrative mechanisms for direct patient payments to providers: When copayments and coinsurance are owed, such as for specialist visits and pharmaceuticals, patients never pay providers directly. Instead they use their health plan membership cards to make copayments. The provider then receives the full fee from the health plans, which collect copayments electronically from enrollees’ bank accounts each month.
After-hours care: After-hours care is available via hospital emergency departments (EDs), freestanding walk-in urgent care centers (both nonprofit and for-profit), and physician home visits provided by for-profit companies. The Ministry of Health has overall responsibility for after-hours care, and it has promoted the establishment of urgent care in several localities that are far from hospital EDs.
Primary care physicians are not required to provide after-hours care. They receive reports on their patients from the after-hours providers and, increasingly, this information is conveyed electronically.
All health plans operate national telephone advice lines for their members, staffed by nurses with physician backup. All of Israel’s hospital EDs are connected to the national health information exchange; efforts are underway to link them with community-based urgent care centers as well.
Hospitals: Of the 45 acute care hospitals, 18 are government-owned, either by the Ministry of Health or by municipalities. These account for 57 percent of the national capacity. Another 40 percent of acute care beds are operated by 16 private nonprofit hospitals that are owned by health plans or nonprofit organizations. Eleven for-profit hospitals account for the remaining 3 percent of bed capacity. These tend to be smaller hospitals that specialize in elective procedures.12
Reimbursement of hospital care varies:
- Hospital emergency care is reimbursed on a fee-for-service basis.
- Inpatient medical care is reimbursed on a per-diem basis.
- Inpatient procedures are paid either per diem or through activity-based, procedure-related group (PRG) arrangements.13
- Outpatient care is reimbursed on either a fee-for-service or a procedure-related group basis.
Maximum payment rates are set by the government, but health plans negotiate discounts. The government also sets revenue parameters (minimum and maximum), which limit the extent to which each hospital’s total revenues can decrease or grow from year to year. Hospital payments cover all costs, including the cost of the physicians. Procedure-related group payments include all costs of a hospitalization episode, excluding rehabilitation. There are no extra payments for severity, outliers, expensive treatments, or the adoption of new technologies.
Government and nonprofit hospitals follow a national hospital fee schedule, but for-profit hospitals’ prices are unregulated. Fee-for-service is the predominant payment mode for private for-profit hospitals.
In government and nonprofit hospitals, physicians are predominantly salaried employees, with limited arrangements for supplemental fee-for-service payments for procedures performed outside regular hospital hours.
Until 2018, there was largely no choice of specialist in nonprofit hospitals. Patients wishing to choose a specialist or surgeon had to go to a for-profit hospital and pay out of pocket or use voluntary health insurance. Since 2018, some large public hospitals have started offering free choice of surgeon.
Mental health care: In 2015, responsibility for the provision of mental health care was transferred from the Ministry of Health to the NHI health plans, which provide care through a mix of salaried professionals, contracted independent professionals, and purchased services. The Ministry of Health continues to own and operate community-based mental health clinics, which are now under contract with the health plans.
NHI-mandated mental health coverage is broad and includes psychotherapy, medications, and inpatient and outpatient care. Integration of mental health and medical services is currently limited but is expected to improve because of the transfer of responsibility to the health plans. Psychologists are the main source of professional mental health care for half of patients, and psychiatrists and primary care physicians serve a quarter of patients.14
Since the health plans took over mental health care, the availability of community-based services has increased substantially. However, there are still significant waiting times, particularly for psychotherapy and child psychiatry. These delays are due in part to shortages of some types of mental health professionals and to the health plans’ difficulties in attracting and contracting with professionals, who can earn much more in the private sector.
Long-term care and social supports: Long-term care is not covered by NHI, but is covered separately. The government publicly funds long-term care services through general taxes.
In 2014, 86 percent of adults age 65 and older with disabilities received community-based long-term care, while the remaining 14 percent received institutional long-term care.15 Community-based services account for 52 percent of total long-term care expenditures, of which 67 percent was publicly funded.16
Approximately half of the adult population purchases private long-term care insurance.17
Institutional long-term care financing is subsidized by the Ministry of Health and is awarded based on needs and means tests. These subsidies are generally paid directly to providers, although families can receive cash subsidies to pay providers.
Community-based long-term care is funded by the National Insurance Institute, and eligibility is based on needs and means tests. It includes personal care and housekeeping services for community-dwelling seniors with disabilities.18 In addition, the National Insurance Institute covers an extensive network of daycare centers and a growing network of supportive neighborhoods. An emergency call service, physician home visits, and social activities are also covered. Additionally, in every community, a facilitator coordinates social supports and apartment repairs.
Until 2018, there was no financial support for informal or family caregivers; there are means-tested government subsidies for home aids.
NHI health plans are responsible for providing medical care, such as home nursing care, for the disabled elderly living in the community. In recent years, they have increased access to clinicians (particularly for the homebound elderly) via home care teams and telemedicine.
About two-thirds of nursing home care and nearly all home aids are provided by private, for-profit companies, with the remainder being public.
Hospice care is a mandated NHI benefit. In practice, however, while some hospice care is available, particularly home hospice, there is considerable unmet need.
What are the major strategies to ensure quality of care?
Israel has a well-established system for monitoring the quality of primary care. Comparative quality data for individual health plans has been made public since 2014.19 While the published data relate to the health plans at the national level, the plans also maintain internal data on regions, clinics, and individual physicians.20 Plans monitor the care provided by their GPs and work closely with them to improve quality.21
The Ministry of Health publishes comparative, hospital-specific quality data. The number of quality indicators and of the types of services covered has been growing rapidly. Currently, explicit financial incentives for hospitals to improve quality exist only for timely care of hip fractures or stroke.
The Ministry of Health also has a well-developed system for monitoring the quality of care in nursing homes and mother-and-child clinics, and is sharing this performance information with the public. There is no parallel system for home care services.
Practice guidelines exist for some clinical areas. These have been developed by professional medical associations, often in collaboration with the Ministry of Health.
All Israeli general hospitals are required to have received, or to be working toward, accreditation by Joint Commission International. As of June 2018, almost all of the general hospitals were accredited.
An independent research institute carries out biannual surveys of the general population regarding the service level provided by NHI health plans and the level of satisfaction with the health system. The Ministry of Health recently launched an annual survey of hospitalized patients, publishing results for individual hospitals.
National registries are maintained by the Ministry of Health for certain expensive medical devices and for a broad range of diseases and conditions, including cancer, low birth weight, trauma, and occupational diseases.
What is being done to reduce disparities?
The Ministry of Health is leading a major national effort to reduce disparities, in cooperation with the NHI health plans and hospitals.22 Key initiatives include:
- Reducing financial barriers to care, particularly for those with low incomes and other vulnerable populations. Most prominently, mental health and dental care for children and the elderly have been added to the NHI benefit package.23
- Enhancing the availability of services and professionals in remote regions by increasing the supply of beds and technologically advanced equipment in those regions.
- Addressing the unique needs of minorities through the adoption of cultural responsiveness requirements for all providers, the establishment of a national translation call center, and targeted interventions for the Bedouin and other high-risk groups.
- Implementing intersectoral efforts to address the social determinants of health and promote healthy lifestyles.
What is being done to promote delivery system integration and care coordination?
The four NHI health plans are essentially the main source of primary, specialty, and mental health care. This structural integration provides a foundation for providing relatively seamless care, including care for complex and chronically ill patients. The plans’ health information systems link primary and specialty care providers, and a new national health information exchange is adding hospital data to this system. These systems are increasingly providing access to electronic patient information at the point of care.
In addition, the health plans have established several targeted care management programs that aim to provide comprehensive integrated care for complex patients with chronic conditions. These make extensive use of the plans’ sophisticated information systems, videoconferencing, and other innovative techniques.24
What is the status of electronic health records?
All health plans have electronic health record (EHR) systems that link all community-based providers: primary care physicians, specialists, laboratories, and pharmacies. All GPs work with EHRs. Hospitals are also computerized but are not fully integrated with health plan EHRs. The Ministry of Health is leading a major national health information exchange project to create a system for sharing relevant information across all hospitals and health plans.
Each citizen has a unique patient ID. Patients have the right to get copies of their medical records from hospitals and health plans, and patients can book appointments and access many components of their EHR online (such as lab test results), but full records are not generally available. Efforts are underway to set up secure messaging systems linking patients and their GPs.
How are costs contained?
Among high-income countries, Israel is one of the most successful at containing costs. Strategies include:
- Instituting tight control of resources and expenditures. About half of national health expenditures are channeled through the Ministry of Finance.25 There are rigorous controls on key supply factors, such as hospital beds and expensive medical equipment, as well as physician and nurse positions in hospitals. In addition, the government sets maximum reimbursement rates and global revenue caps for hospitals.
- Using various managed care approaches. The NHI health plans essentially work as managed care organizations, providing care within budgets that are largely determined prospectively by capitation. The plans employ a variety of mechanisms for controlling utilization and costs, such as purchasing pharmaceuticals in bulk and incentivizing the use of generics. Health plans also maintain a well-developed system of prevention and community-based services to reduce reliance on high-cost hospital care.
- Explicitly prioritizing public funding for new technologies included in the NHI benefit package.
- Deploying risk-sharing agreements for certain high-cost drugs. The pharmaceutical companies fund patients’ drugs after a predetermined supply has been depleted.
- Implementing demand-side levers, including cost-sharing for specialist visits and coinsurance for pharmaceuticals, with higher rates for patented medications.
- Aligning organizational and financial incentives between clinicians and the hospitals or health plans for which they work. For example, health plans have various internal processes for discouraging the delivery of care that provides poor value.
What major innovations and reforms have recently been introduced?
A number of innovations have been launched in recent years, including the following:
- Creating an environment to encourage healthy diets. The Ministry of Health has imposed measures such as mandatory food labelling and restrictions on advertising unhealthy food for children. It has been incentivizing food manufacturers to produce healthier products, and has been improving economic access to healthy food through the taxation of unhealthy food. In addition, the Ministry of Health is improving the nutritional value of food served in public institutions, and is including education on healthy diets in the school curriculum for young children.26
- Expanding the role of nurses in the community. In 2018, the Ministry of Health extended the responsibilities and scope of practice for specialist nurses in the community, to relieve some of the pressure on primary care physicians. Specialist nurses can now treat mild cases of acute diseases and cases that are urgent but simple to treat; treat and monitor patients with chronic diseases; provide preventive care and handle health promotion; and prescribe medications and contraceptives. Specialist nurses can also provide palliative care and refer patients for diagnostic tests, to specialists, and to EDs.27
- Improving continuity of care. Urgent care centers are required to report patient data (diagnosis, treatment, recommendations for future care) to the patient’s health plan and to the hospital if the patient is referred for acute care, bridging the information gap between community and inpatient care. Centers must also report cases of communicable or rare diseases and domestic violence to relevant authorities.28
- Further expanding dental care coverage. The 2018–2019 Ministry of Health budget funds the expansion of the health basket to include dental care for people aged 75+ during 2018, and for children up to 18 years old during 2019. This step concludes the “reform of dental care for children,” which started in 2010 with the inclusion of dental care for children up to 8 years of age to the health basket.29
- Increasing the scope, breadth, and depth of services for older people. To better meet the needs of Israel’s aging society, the Ministry of Health is broadening eligibility for long-term care.30